Compartment Pressure Testing
What is Compartment Pressure Testing?
Compartment pressure testing is a method of testing the pressure inside the different compartments of the leg or arm.
When is Compartment Pressure Testing Performed?
When there is exertional leg pain (usually during sport or running), compartment pressure testing can help determine whether or not there is Chronic Exertional Compartment Syndrome (CECS). It is also used to exclude Acute Compartment Syndrome after trauma and fractures. Compartment syndrome can also happen in the forearms , usually in highly active athletes training and competing in Kayaking, Rowing, Mixed Martial Arts and Weight Lifting.
Exertional leg pain can be very difficult to diagnose and often requires advanced expertise.
There are often multiple, overlapping sources of pain, including:
- Compartment Syndrome
- Medial Tibial Stress Syndrome and Stress Fractures
- Vascular Insufficiency (Popliteal Artery Entrapment Syndrome)
- Nerve Entrapments
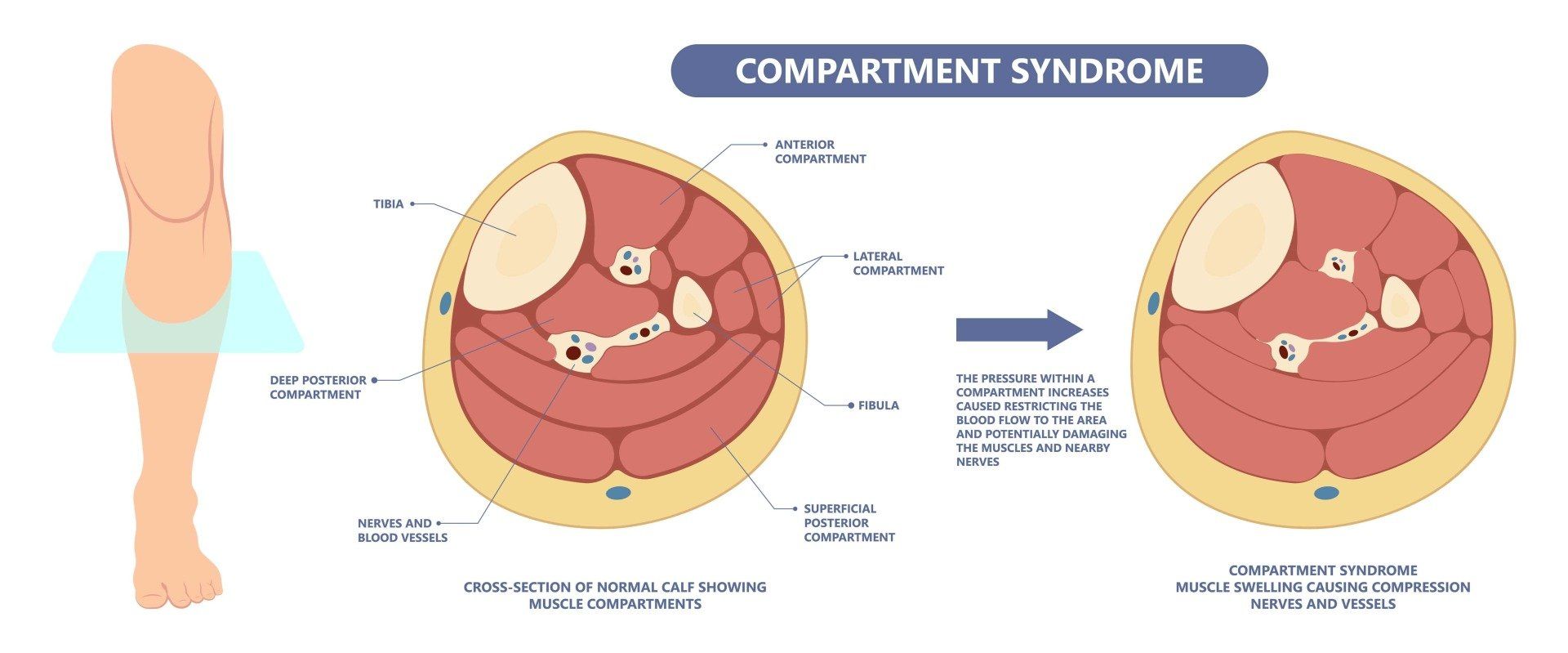
What is Compartment Syndrome?
Chronic exertional compartment syndrome (CECS) is a condition that causes cumulative, crescendo-like pain in the legs during exercise. This is thought to be caused by excessive stiffness of the layer of tissue that wraps the muscles in the legs, called the fascia. Muscle increases its volume by 200% during exercise, due to increased blood flow, and if the fascia is too tight, it literally strangles the muscle and starves it of oxygen. This leads to pain that worsens during exercise but is usually relieved with rest.
In very rare cases, acute and unaccustomed exercise (or acute trauma such as fractures) can lead to Acute Compartment Syndrome, where the pressure is not relieved by rest, and urgent surgical decompression is required.
How is Compartment Pressure Tested?
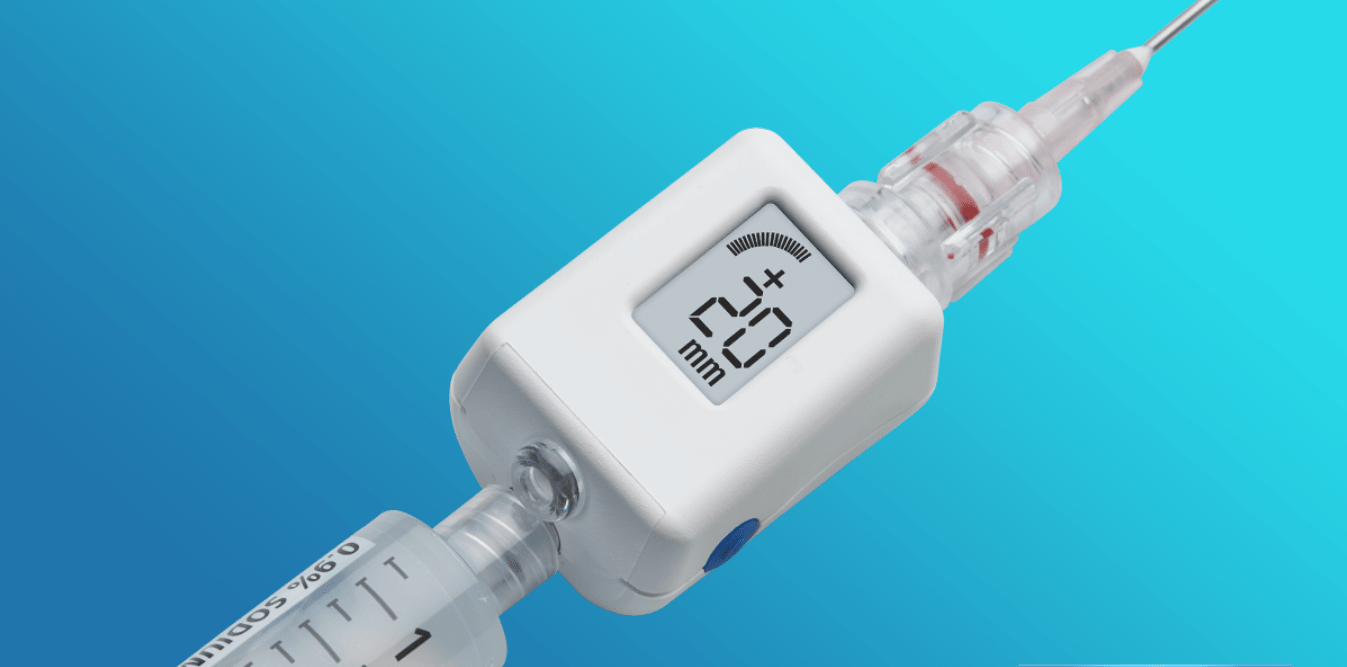
Compartment pressure is tested using a pressure transducer attached to a needle. After local anaesthetic is injected into the spots that these needles will pass into the affected compartments of the leg, the patient is asked to exert themselves (usually on a treadmill), until their pain comes on and for a further few minutes to ensure they are present when the compartments are tested at 1 minute and 5 minutes after exertion. See the below animation to see how the procedure is performed.
A positive test is confirmed and a diagnosis of Exertional Compartment Syndrome of 1 or more specific leg compartments (anterior, lateral, deep posterior) is made when the pressure is over 25mmHg at any time, over 30mmHg at 1 minute or over 20mmHg at 5 minutes. Normal pressures at rest are under 10mmHg.
Differential Diagnosis of Leg Pain
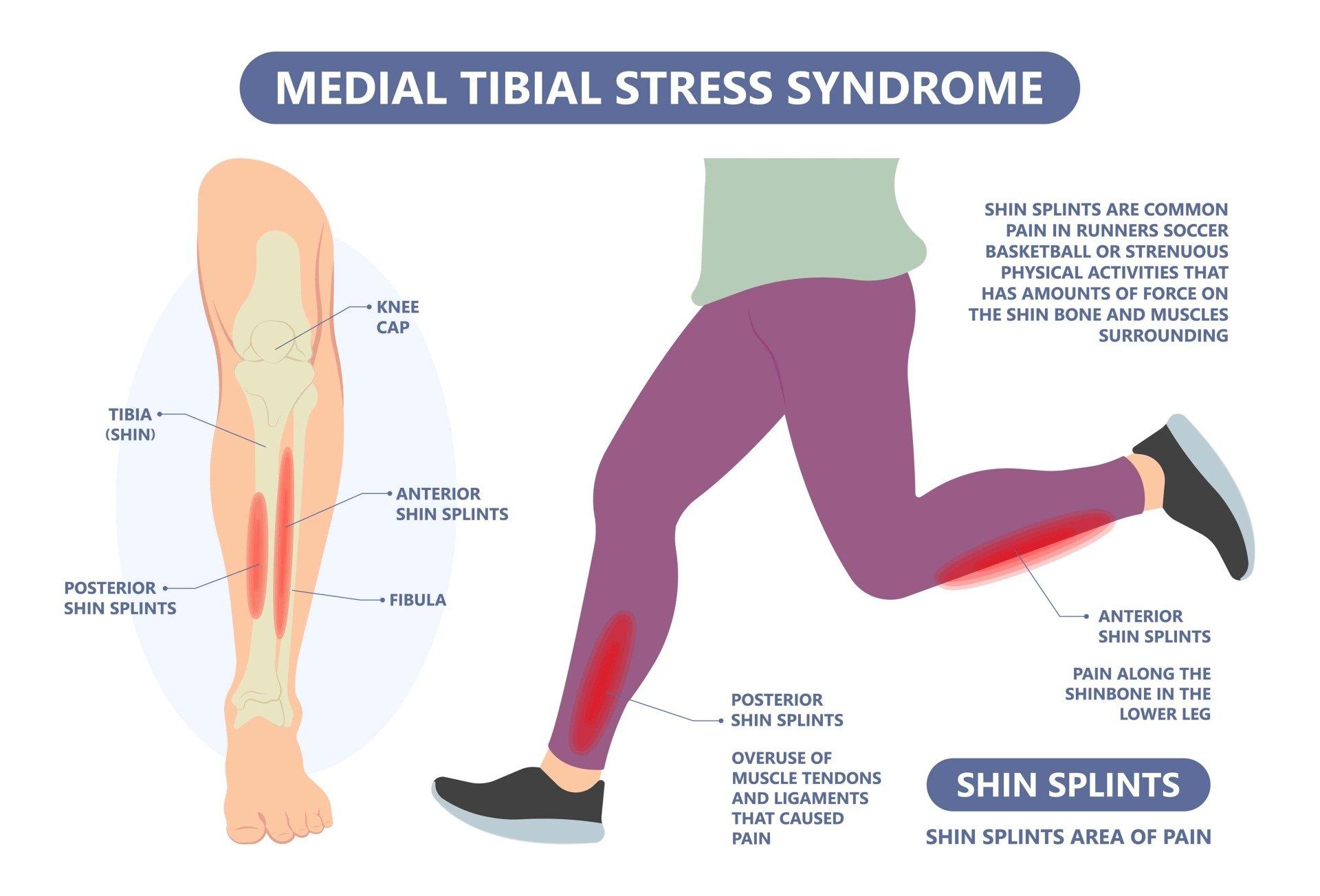

Other causes of Exertional Leg pain include Medial Tibial Stress Syndrome (Shin Splints), Popliteal Artery Entrapment Syndrome and Nerve Entrapments.
Medial Tibial Stress Syndrome (MTSS) causes pain that tends to radiate down the inner shins. There is often a history of gradual onset with rapidly increasing training loads or training errors. There may be biomechanical factors such as hard surfaces, inappropriate footwear, flat feet or high arches, and poor pelvic stability. While the overall mechanical cause is the same, there is a spectrum of severity from simple “Shin Splints”, which only affects the soft tissues, to a full-blown Stress Fracture that requires rest and rehabilitation.
Popliteal Artery Entrapment Syndrome (PAES) tends to occur in Sprinters with larger calf muscles due to occlusion of the popliteal artery that supplies the calf (usually by the medial head of gastrocnemius calf muscle). It can appear very similar to CECS because it also affects the blood flow to the muscle. However, key differences include a more rapid onset with intense exercise, more rapid relief of pain with rest, and less cumulative pain when exertion is repeated. Point of care ultrasound showing complete occlusion of the popliteal artery can be very suggestive during dynamic manoeuvres (especially if symptoms are reproduced). A CT angiogram or MRI scan with contrast, with the toe being pointed during the scan, often provides definitive evidence for entrapment.
Nerve Entrapments are rare but can occur with trauma, post-operative scar tissue or injury. The superficial peroneal nerve and common peroneal nerve are the most common causes of nerve entrapment and can be assessed by dynamic ultrasound in the context of the history and examination.
A full history and clinical examination must be undertaken to assess the likely source of pain, as well as the underlying contributors.
The location of the pain, history of onset and pattern of relief and associated features of numbness will direct the further assessment. A comprehensive neurological and vascular examination, along with dynamic ultrasound can then narrow the source of pain.
Features of CECS include worsening pain with exertion (particularly running), localisation of the pain to the side, front or back of the legs, muscle herniation and tingling or numbness of the feet. All of this relates to the restriction of blood flow to the affected compartment. About 80% of cases affect BOTH legs.
We know that capillary blood flow is compromised when the pressure in the compartment is within 30mmHg of the diastolic pressure. The “Delta Pressure” is a calculation of this, and determines the risk of muscle death (myonecrosis) if the compartment pressure is not treated.
Treatment - Do I Need Surgery?
Treatment for Exertional Leg Pain depends on the diagnostic entities AND the intrinsic and extrinsic contributors to the pain.
Not every patient with Chronic Exertional Compartment Syndrome requires surgery, since changes to footwear, activities, body weight and running biomechanics can changes symptoms markedly.
A
running biomechanical assessment
is strongly recommended in runners who have this condition prior to considering surgery. Physiotherapists like Alex Bell who specialise in this area are instrumental to recovery, whether or not surgery is required.