Is a cortisone injection the right choice for you?
As a Sport & Exercise Medicine Physician, I use ultrasound-guided cortisone injections selectively — only where the diagnosis is clear and the inflammation is genuinely the problem. Here’s an honest guide to help you decide.

What is a cortisone injection?
Cortisone is a synthetic form of cortisol, a hormone your body makes naturally to help regulate inflammation. As an injection it is a potent anti-inflammatory that reduces pain, swelling and stiffness.
The key thing I explain to every patient is that cortisone is a catabolic steroid — it calms tissue down rather than building it up. That makes it powerful for settling inflammation, but it also means it does not heal the underlying injury. Its real value is buying a window of relief so that rehabilitation can do the lasting work.
My approach is simple: the injection is only as good as the diagnosis behind it. I’d rather talk you out of an injection you don’t need than give you one that could set your recovery back.
Where cortisone helps — and where we’re cautious
Cortisone is a tool, not a cure. Used in the right problem it is excellent; used in the wrong one it can do more harm than good. Here is how we decide.
Inflammatory & compressive problems
Cortisone is at its best where excess inflammation is the main driver of pain.
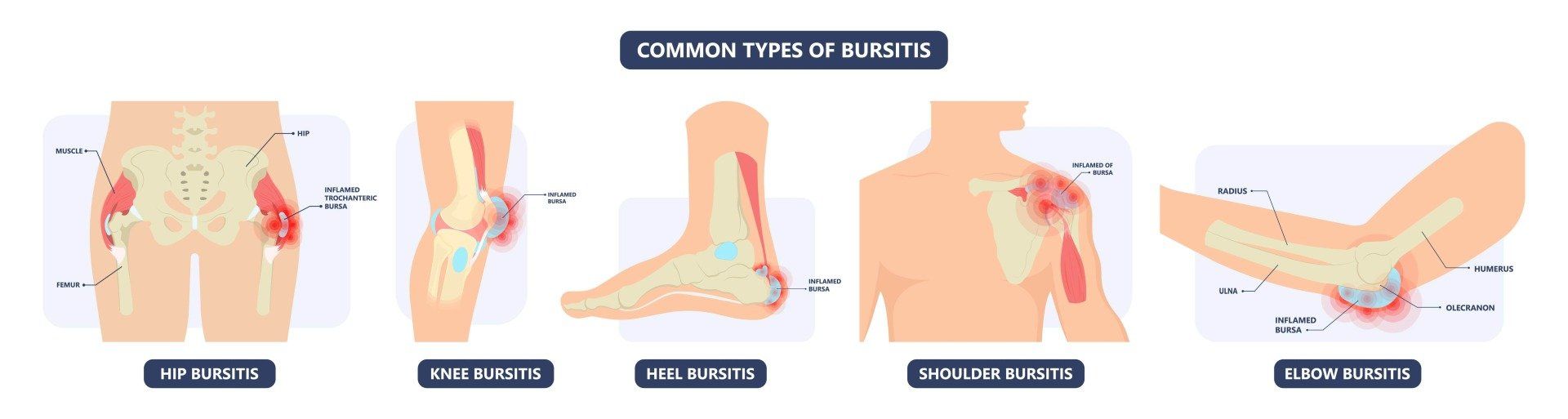
- Inflamed bursae – e.g. subacromial (shoulder), trochanteric (hip), olecranon (elbow), retrocalcaneal (heel)
- Frozen shoulder and shoulder impingement
- Joint osteoarthritis flares (knee, hip, thumb base, facet joints)
- Carpal tunnel syndrome
- Lumbar nerve-root irritation (“sciatica”)
- Acutely swollen, painful sprains where inflammation is limiting rehab
- Hoffa’s (knee fat-pad) impingement
Chronic tendon & load-related problems
Here cortisone may ease pain briefly but can worsen 12-month outcomes — better options usually exist.
- Chronic tendinopathy – tennis elbow, Achilles, patellar tendon
- Direct injection into a tendon (risk of weakening and rupture)
- Where infection is suspected at the site
- As a substitute for loading-based rehabilitation
- Repeated injections into the same weight-bearing joint or tendon
Precise, ultrasound-guided, minimally invasive

Prepare & numb
The skin is cleaned with antiseptic. A fine needle is used and local anaesthetic is usually mixed with the cortisone.
Guide with ultrasound
Unless the target is very superficial, ultrasound guides the needle precisely into the structure causing your pain.
Deliver & rest
The cortisone is delivered accurately. You’ll rest the area — strictly for 24 hours — while it takes effect.
Bursitis & other inflammatory problems
An inflamed bursa — a small fluid-filled cushion near a joint — is one of the conditions that responds most reliably to a cortisone injection. Bursitis is common at the hip, knee, heel, shoulder and elbow.
What an ultrasound-guided injection involves
Swipe through the key elements — from the live ultrasound image to the conditions we treat.

Ultrasound-guided accuracy
A live ultrasound image lets us place the needle precisely into the target structure, rather than relying on landmarks alone.

A fine needle, local anaesthetic mixed in
The needle is thin and local anaesthetic is usually combined with the cortisone, so most people describe only brief pressure or a mild sting.
Common bursae we treat
Inflamed bursae at the hip, knee, heel, shoulder and elbow are among the conditions that respond most reliably to a corticosteroid injection.
What the research tells us
Cortisone reliably reduces inflammatory pain in the short term. The most important nuance is timing: for chronic tendon problems, the early relief can come at the cost of poorer recovery months later, so injection is rarely the first choice there.
This is why a careful diagnosis matters more than the injection itself — getting the indication right is what determines a good outcome.
Key references: Bisset L et al., corticosteroid injection vs exercise vs wait-and-see for tennis elbow (BMJ, 2006); Coombes BK et al., corticosteroid injection and lateral epicondylalgia outcomes (JAMA, 2013). General guidance only — not a substitute for individual medical advice.
Not sure cortisone is right for you?
For chronic tendon and joint problems we often recommend regenerative or lubricating options instead. Explore the alternatives:
Cortisone injection FAQs
If you have a question specific to your treatment, we recommend contacting the clinic.
For inflammatory and compressive problems — bursitis, frozen shoulder, carpal tunnel, nerve-root pain, osteoarthritis flares — cortisone can give fast, meaningful relief lasting several weeks to around three months.
For chronic tendon problems the picture is different. Randomised trials in tennis elbow show that while a cortisone injection helps in the first few weeks, patients can do worse at 12 months than those who simply waited or did exercise-based rehab. For these conditions we usually recommend other options first.
A corticosteroid (cortisone) — a synthetic version of cortisol, the hormone your body makes naturally. Common preparations include triamcinolone, methylprednisolone or betamethasone. It is a potent anti-inflammatory.
In most cases a small amount of local anaesthetic is mixed in. This numbs the area quickly and confirms the needle is in the right place. Cortisone reduces pain, swelling and stiffness — but it is important to understand it does not heal damaged tissue; it creates a calmer window for rehabilitation to work.
Cortisone injections are very safe when done well, but no procedure is risk-free. Specific points to know:
Infection and bleeding are rare (in the order of 1 in 80,000 injections). Post-injection flare — a temporary increase in pain for 24–48 hours — is the most common effect.
Less commonly: facial flushing, and short-lived mood, sleep or menstrual changes (more likely if you’ve had them before). Shallow injections can cause skin lightening (depigmentation) or a small dimple of fat thinning, especially in darker skin. Tendon rupture can occur if cortisone is injected directly into a tendon — which is why we avoid that. People with diabetes may notice a temporary rise in blood-sugar for a few days.
If pain at the site persists beyond a couple of days, or you develop fever, spreading redness or heat, please contact the clinic for review.
Often a single, well-placed injection is enough to settle a flare and let rehabilitation progress. Some conditions benefit from a second injection after review.
We deliberately avoid repeated injections into the same tendon or weight-bearing joint, because cortisone is a “catabolic” steroid that can weaken tissue over time. As a general guide we limit injections at any one site, and we’ll always discuss the trade-offs with you.
0–4 hours: the area feels numb from the local anaesthetic. 24–48 hours: a possible flare in pain — rest and ice. 3–7 days: the cortisone takes effect and pain settles. Weeks to ~3 months: your window of relief.
Plan to rest the injected area — strictly for the first 24 hours, and ideally for 5–7 days for a weight-bearing or tendon-related site. Depending on the area you may need someone to drive you home, or to wear a sling or boot. Use this calmer window to progress your rehabilitation.
Tell us if you take aspirin, anti-inflammatories or blood-thinning medication — whether or not an injection is planned. In the 24 hours before, avoid large amounts of alcohol and vigorous exercise, and wear loose, comfortable clothing.
Your doctor will take a history, examine you, and may arrange tests or imaging to confirm the injection is the right step and the safest target.
Discomfort is usually mild. The needle is fine and local anaesthetic is generally mixed in, so most people feel a brief sting or a sensation of pressure that passes quickly.
Once the anaesthetic wears off (about 2–4 hours later) some people notice a temporary “post-injection flare” for 24–48 hours. This settles with rest and ice, and responds well to simple pain relief.
Let us know early. Corticosteroid injections are generally deferred during pregnancy and used only when clearly necessary, after weighing the benefits and risks with you. Small amounts are considered low-risk in breastfeeding, but we’ll always discuss your individual situation first.
Cortisone injections in children and adolescents are uncommon and are decided case-by-case, with attention to growth plates and developing tendons. They are arranged only where genuinely indicated and after a specialist assessment.
Talk through your options with Dr David Samra
Book an assessment to find out whether a cortisone injection — or a different approach — is the best next step for your injury.
121 Norton Street, Leichhardt NSW 2040
Reference List
1. Bisset L, Beller E, Jull G, Brooks P, Darnell R, Vicenzino B. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. BMJ. 2006 Nov 4;333(7575):939.
2. Coombes BK, Bisset L, Vicenzino B. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials. Lancet Lond Engl. 2010 Nov 20;376(9754):1751–67.
3. Dean BJF, Lostis E, Oakley T, Rombach I, Morrey ME, Carr AJ. The risks and benefits of glucocorticoid treatment for tendinopathy: a systematic review of the effects of local glucocorticoid on tendon. Semin Arthritis Rheum. 2014 Feb;43(4):570–6.
4. Nichols AW. Complications associated with the use of corticosteroids in the treatment of athletic injuries. Clin J Sport Med Off J Can Acad Sport Med. 2005 Sep;15(5):370–5.
5. Hart L. Corticosteroid and other injections in the management of tendinopathies: a review. Clin J Sport Med Off J Can Acad Sport Med. 2011 Nov;21(6):540–1.
6. Wu T, Song HX, Dong Y, Li JH. Ultrasound-guided versus blind subacromial-subdeltoid bursa injection in adults with shoulder pain: A systematic review and meta-analysis. Semin Arthritis Rheum. 2015 Dec;45(3):374–8.
7. Habib GS, Badarny S, Rawashdeh H. A novel approach of local corticosteroid injection for the treatment of carpal tunnel syndrome. Clin Rheumatol. 2006 May;25(3):338–40.
8. Manchikanti L, Cash KA, Pampati V, Falco FJE. Transforaminal epidural injections in chronic lumbar disc herniation: a randomized, double-blind, active-control trial. Pain Physician. 2014 Aug;17(4):E489–501.